
Compare
BunnyCDN Pricing in 2026: What You Actually Pay per TB
Imagine a bustling global marketplace where digital content flows as smoothly as traffic in a well-orchestrated city. ...
Fewer than 5% of adult cancer patients in the United States enroll in a clinical trial. That number has barely moved in two decades, despite billions poured into recruitment infrastructure. The bottleneck is not willingness. It is matching: parsing thousands of active protocols against a patient's molecular profile, treatment history, comorbidities, and real-time lab values, then surfacing actionable options before the therapeutic window closes. AI clinical trial matching, as implemented by Tempus and a small cohort of competitors in 2026, directly attacks this bottleneck. This article breaks down the architecture Tempus uses, benchmarks the measurable impact on enrollment velocity, introduces a decision framework for evaluating clinical trial matching platforms, and examines the failure modes that engineering and clinical teams should plan for.
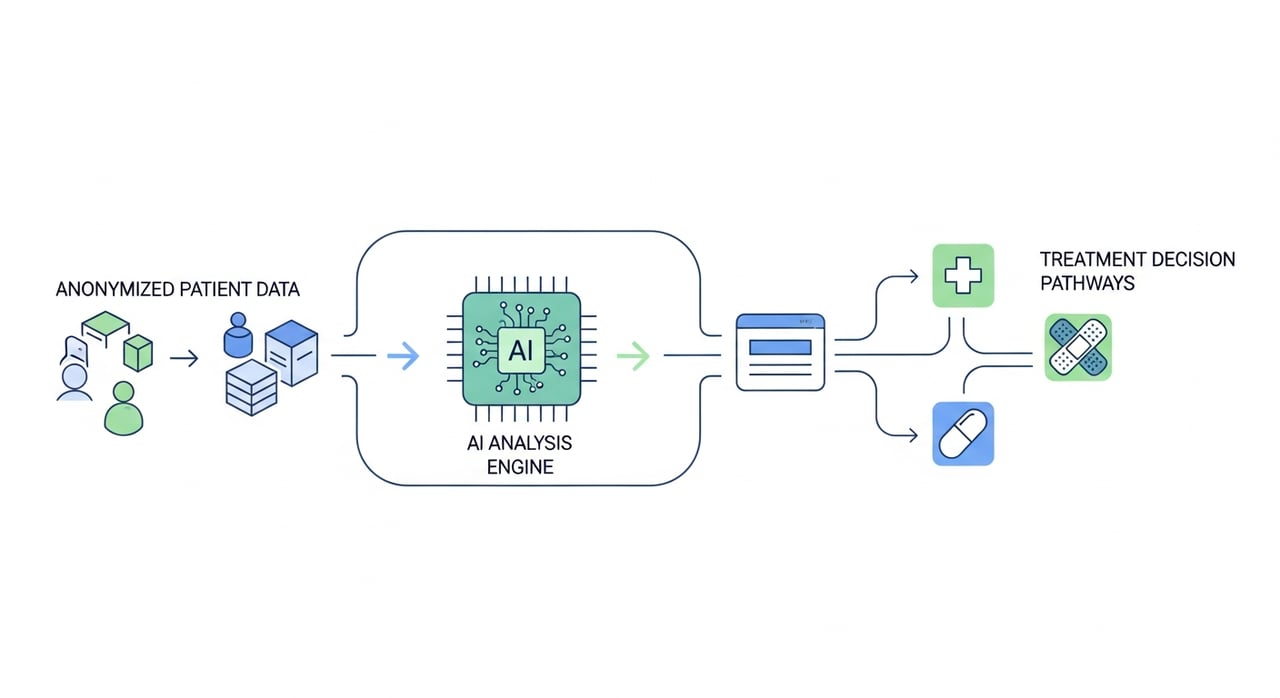
Tempus operates on a data layer that, as of Q1 2026, aggregates de-identified clinical records from over 7,000 oncologists and hundreds of health systems across the US. The matching pipeline ingests structured EHR fields (ICD-10 codes, medication lists, lab panels) alongside unstructured data: pathology narratives, radiology reports, and clinician notes. A combination of NLP extraction models and proprietary ontology mapping normalizes this heterogeneous input into a patient feature vector.
That vector is then evaluated against a continuously updated index of active trial eligibility criteria. Tempus parses ClinicalTrials.gov protocols programmatically, but the real differentiator is their manual curation layer: a team of clinical data abstractors resolves ambiguous inclusion/exclusion language that pure NLP still mishandles. The result is a ranked list of trial matches delivered inside the EHR workflow, typically within the oncologist's existing Epic or Cerner session.
What separates Tempus from legacy screening logs is the molecular axis. Tempus xT, their 648-gene panel (expanded from 596 genes in late 2025), produces somatic mutation, copy number alteration, and fusion data that feeds directly into eligibility evaluation. A patient with a KRAS G12C mutation, for instance, is automatically surfaced for trials targeting that variant. This eliminates the manual cross-referencing that historically added days or weeks to the screening process.
Whole transcriptome sequencing data and, as of 2026, methylation profiling results are also factored into matching where trial protocols specify molecular subtypes. The integration is bidirectional: Tempus feeds trial enrollment outcomes back into its models to refine match-quality scoring over time.
Trial matching is the entry point, but the Tempus platform extends into treatment-decision support. Their algorithmic therapy recommendation engine, Tempus TO (Therapy Overview), synthesizes a patient's molecular data against published evidence and real-world outcomes from Tempus's own dataset. In Q1 2026, Tempus disclosed that TO recommendations are generated for over 60% of sequenced patients within 48 hours of report finalization.
This is not a replacement for tumor board deliberation. It is a pre-processing step that ensures the treating oncologist walks into that discussion with a ranked set of evidence-backed options, including relevant clinical trials, rather than relying on memory or ad hoc literature searches.
On the sponsor side, Tempus provides predictive enrollment modeling. Using historical accrual data and real-time screening rates, their platform forecasts site-level enrollment trajectories. This allows sponsors to reallocate budget to high-performing sites or activate new sites before enrollment stalls, rather than reacting months after a shortfall becomes visible in the data.
As of 2026, Tempus reports a median time-to-first-patient enrolled that is 35% shorter than the industry benchmark for Phase II oncology trials. That figure is self-reported and should be interpreted with the usual caveats, but it aligns with independent observations from large academic medical centers using the platform.
Tempus is not the only player. Deep 6 AI, TrialJectory, Massive Bio, and several health-system-built tools compete in this space. For engineering and clinical informatics teams evaluating options, the following framework captures the dimensions that actually matter in production:
| Evaluation Dimension | What to Measure | Tempus (2026 Status) |
|---|---|---|
| EHR Integration Depth | Structured + unstructured data ingestion; in-workflow delivery | Epic/Cerner native; NLP on free text; results in EHR |
| Molecular Data Utilization | Panel size, data types (SNV, CNV, fusions, RNA, methylation) | 648-gene panel; WTS; methylation as of 2026 |
| Criteria Parsing Accuracy | False-positive and false-negative match rates against manual screen | Hybrid NLP + human curation; published precision above 85% |
| Feedback Loop | Does enrollment outcome data retrain the matching model? | Yes; closed-loop retraining confirmed |
| Regulatory Posture | HIPAA, SOC 2, state-level privacy law compliance | HIPAA-compliant; SOC 2 Type II; de-identification pipeline |
| Sponsor-Side Analytics | Enrollment forecasting, site performance dashboards | Real-time accrual prediction; site rebalancing tools |
The dimension most teams underweight is criteria parsing accuracy. A platform that surfaces 200 matches with 40% false positives generates more coordinator burden than it eliminates. Demand published precision/recall numbers, and ideally run a shadow evaluation against your own screening logs before committing.
No coverage of AI clinical trial matching is complete without addressing where these systems break. Three failure patterns recur across deployments:
1. Stale protocol indexing. Trials amend eligibility criteria mid-enrollment. If the matching platform lags ClinicalTrials.gov updates by even a few days, patients get matched to criteria that no longer exist. Tempus claims daily protocol synchronization as of 2026, but downstream curation latency can add 24-72 hours. Ask about amendment propagation SLAs.
2. NLP extraction errors on edge-case narratives. Pathology reports from smaller labs, handwritten addenda, or non-standard abbreviations still trip extraction models. A patient whose EGFR status is buried in a free-text addendum rather than a structured field can be missed entirely. Institutions deploying these tools should audit match lists against a random sample of charts quarterly.
3. Consent and workflow friction. The AI identifies a match; the coordinator calls the patient; the patient has already started a new line of therapy, moved out of state, or declined trials previously. Matching quality is necessary but insufficient without a fast, low-friction consent workflow integrated into the patient-facing experience. Tempus has invested here with their patient portal, but the gap between algorithmic match and signed consent remains the largest source of lost enrollment.
Platforms like Tempus generate and transfer substantial volumes of genomic data, imaging files, and analytic payloads between sequencing labs, cloud compute environments, and clinical endpoints. The delivery infrastructure underneath matters. Latency spikes or transfer failures during result delivery can push a match notification outside the treatment-decision window. For organizations building or operating similar data-intensive healthcare pipelines, cost-effective and fault-tolerant content delivery is a real engineering concern. BlazingCDN's enterprise edge configuration offers stability and fault tolerance on par with Amazon CloudFront at a fraction of the cost, starting at $4 per TB for lower volumes and scaling down to $2 per TB at 2 PB+. For healthcare and life sciences organizations transferring large genomic datasets and analytic reports at scale, that cost differential compounds fast.
AI systems ingest structured and unstructured EHR data, molecular profiling results, and protocol criteria simultaneously, then produce ranked matches in minutes rather than the days or weeks required for manual chart review. The primary gain is coverage: AI can evaluate a patient against thousands of active protocols, whereas a coordinator typically screens against a handful of trials they are aware of at their site.
Tempus combines structured EHR fields (diagnoses, medications, labs), unstructured clinical notes parsed via NLP, and molecular data from their own sequencing panels (xT 648-gene panel, whole transcriptome, methylation profiling as of 2026). Protocol eligibility criteria are sourced from ClinicalTrials.gov and curated by clinical data abstractors.
Yes, though oncology remains the most mature use case because molecular profiling creates a high-dimensional patient feature space that AI exploits effectively. Tempus has expanded into neuropsychiatry and cardiology, and competitors like Deep 6 AI operate across a broader therapeutic range. The matching architecture generalizes; the limiting factor is the richness of available molecular and clinical data per therapeutic area.
Any system that ingests EHR data must operate under HIPAA's minimum necessary standard and maintain BAAs with each health system. Tempus uses a de-identification pipeline for its aggregate research dataset and processes identified data only within the treating institution's authorized environment. SOC 2 Type II certification and encryption at rest and in transit are baseline requirements. Institutions should also verify compliance with state-specific laws such as the California CMIA and Washington's My Health My Data Act, both of which impose obligations beyond HIPAA.
Track three metrics: screen-to-enroll ratio (should decrease), median time from order-to-match-notification (should be under 48 hours), and incremental enrolled patients per quarter attributable to AI-surfaced matches. Compare against your baseline manual screening numbers. A platform that does not move the screen-to-enroll ratio within two quarters is not delivering value regardless of match volume.
If your organization is evaluating or already running an AI clinical trial matching platform, here is a concrete next step: pull your last 90 days of screening logs and calculate your screen-to-enroll ratio, stratified by trial phase and therapeutic area. Then request the same metric from your platform vendor for their aggregate customer base. The delta between your number and theirs tells you whether you have a platform problem or a workflow problem. That distinction determines whether your next investment goes into tooling or into coordinator headcount and process redesign. Share your findings with your clinical informatics team this week; the data ages fast.
Compare
Imagine a bustling global marketplace where digital content flows as smoothly as traffic in a well-orchestrated city. ...

Learn
AWS CloudFront Pricing in 2026: Cost per TB Breakdown At 50 TB/month of egress from US edge locations, your AWS ...

Learn
CDN Failover in 2026: The Five-Nines Architect's Playbook In January 2026, a major European streaming platform lost CDN ...